In case anyone missed it, in May, Florida TV station broadcast a news segment about the link between DES and trassexuality:
http://www.wtsp.com/news/health/can-a-drug-make-you-transgender/215234337I'm wondering if there's any way of building on that success and getting wider coverage for the story. Does anyone here have any ideas?
An interview has just been published with psychologist Dr June Reinisch, who is one of the world's leading experts on the effects of being prenatally exposed to synthetic hormones on people's psychology and behaviour later in life.
http://www.germlineexposures.org/reinisch-qa.htmlThere are some real gems in it which go a long way towards explaining how millions of people ended up being exposed to high doses of DES, even though it was only newly developed and largely untested.
QuoteThere were physicians, particularly ob/gyns, who wanted to do whatever they could do to help women to either get pregnant or stay pregnant. Their treatments were experimental, that is not based on research data but on their clinical understanding of the medications and how they might help their pregnant women who were having difficulty having children. The physicians in general aren't scientists. They're artists. They're the artists of medicine...The doctors took ideas from the drug company detail men, or they came up with their own ideas, but it was not evidence-based – just based upon their own experience and sense of what worked for them.
She also explains why, as an adult, it's often difficult or impossible to establish whether you've been prenatally exposed to pharmaceutical hormones. Medical records very often no longer exist, and even the mothers given the hormones often have no recollection of it afterwards.
QuoteWhen I interviewed these women after the pregnancy, they didn't know what they took—sometimes they didn't remember that they took anything. But I had read their records and I knew what the doctor gave them. I would say, for example, "Don't you remember taking little red pills every day?" "No." They were so focused on being pregnant, maintaining their pregnancy, having the baby, that they had forgotten all about it, including even when they received regular hormone injections. My studies included women who had been taking injections twice a week all the way through their pregnancy. Often they too had no remembrance of it whatsoever. Often the women weren't even told the names of the drugs. It's hard to believe that but it's absolutely true. Or if they were, they did not register.
One other thing that's happened recently is thart I've obtained a copy of a paper in which the testosterone levels of Rhesus monkeys were measured at several points during their prenatal development. The reason for falling back on research on Rhesus monkeys, is that I've gained a strong impression that no one's ever measured the equivalent in human beings. Several times I've seen a chart in which a peak of testosterone occurs at week 17 and then it falls to near zero levels for the remainder of the pregnancy, e.g.
However I have a strong suspicion that researchers have just been requoting the same original decades old source that is not based on actual measurements, but just someone's belief that testosterone during the second half of prenatal development isn't important. There's plenty of first trimester material to work with in the form of aborted and miscarried fetuses, but how do you measure fetal testosterone late in the pregnancy without endangering the baby? You can't, and that's why I have a strong suspicion that no one has ever actually measured it in human beings.
Anyway, the results of the Rhesus monkey research are summarised in this figure taken from the paper:
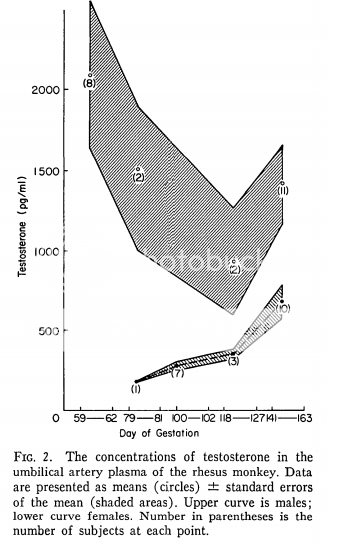
Samples from both male and female fetuses were collected at four points during their fetal development. The first sample (at about day 55) is probably when the monkeys are at a similar point in development to human fetuses around week 17 after conception. You can see that, in males, although testosterone does fall following the peak, it doesn't drop to zero, and it rises again later in gestation. Throughout gestation, male testosterone levels are several times at least higher than in females (although the gap narrows near the due date). It's this difference in testosterone levels that determines whether you get a male or female brain, and I guess the reason females also produce some testosterone is because they need the ability to carry out some male-like behaviours too (just less than in males), so their brains also undergo some masculinisation during normal prenatal development.
Rhesus monkeys are one of the closest animal models to human beings, and I'm sure that the equivalent measurements in humans would show something fairly similar. Now imagine what happens when you throw DES into the mix, at doses more than 10x higher than what will induce complete suppression of testosterone in an adult man (which is what happened during the second half of the pregnancy with DES, when it was administered under the standard dosing schedule for miscarriage prevention that was published annually in the PDR). In a male fetus, instead of being produced at several times the female level throughout the second half of the pregnancy, its production would have dropped to near zero for most or all of that time. As a result, you'd expect to end up with people with highly feminine brains (perhaps even more feminine than an ordinary woman's brain). That does appear to be exactly what's happened too!

