Quote from: KayXo on November 20, 2016, 10:14:03 PM
The cream you used resulted in pregnancy serum levels of progesterone? I recall reading somewhere that eventually the area of application gets saturated and that you no longer absorb P to the same extent. Could that have been the reason? Also, studies have shown that creams yield very low levels of P in the blood.
Who knows what the effect is on serum levels, as I haven't ever had my P levels measured. It's the 10 percent cream though (the strongest one on the market). Like the P creams I've used before, once your body adapts to it, it doesn't have any noticeable effects at all apart from a subtle mood brightening effect. However, it's worth taking, because without it, I get symptoms of estrogen excess (mainly fluid retention, especially in my legs). Also, prior to starting on hormones, I was experiencing some quite alarming neurological symptoms (tinnitus, vertigo, acephalgic migraines), which have stopped since I started taking hormones. I don't know for sure if it't the P that is providing this beneficial effect, but from what I've read about it, it probably is. P has neuroprotective effects and been used experimentally as an antiseizure medication (it's thought to mainly produce these beneficial effects by converting to allopregnanolone, an important neurosteroid).
Quote
In the end, these are all theories and there is no real proof of brain feminization.
Actually there is. The link to ->-bleeped-<- may be contentious, but it's been known for a long time that being prenatally exposed to synthetic estrogens or progestins has permanent, lifelong effects on people's personality and behaviour, that can (and have been) measured in psychological tests.
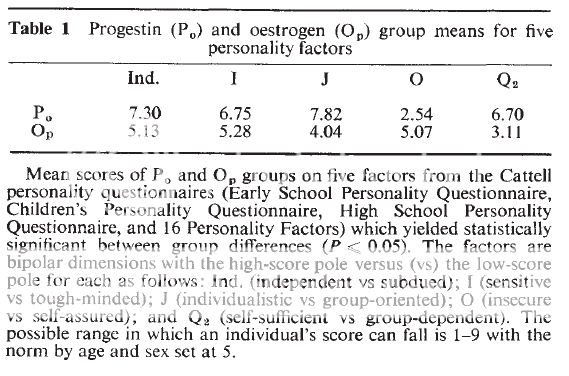
This is from a 1977 study of male and female children who'd been prenatally exposed to synthetic hormones (estrogens, mainly DES, or progestins). The hormone-exposed children were compared with their unexposed siblings as controls, and as you can see, significant differences in the personality traits measured were noted. The main difference in the estrogen exposed group vs controls is that they're more group oriented and group dependent. With the progestin exposed group, they're more independent, more sensitive, strongly individualistic, strongly self assured, and more self sufficient.

This excerpt from the book "Brain Sex", which seems to mainly have had its origin in that study and other similar ones carried out by Dr Reinisch, has articulated what has been left unsaid in those studies. Basically, estrogens tend to induce feminization of behaviour (particularly in males), whereas progestins tend to masculinize it (particularly in females).
Most of the early progestins were androgenic, so it's an open question as to whether pure progestins such as hydroxyprogesterone caproate would act in the same way, and whether their overall effect is masculinizing or feminizing. Also, if I'm right that both DES and progestins inhibit fetal testicular hormone production, then by lumping boys and girls together, a lot of nuances of what has actually happened have been lost, because both types of hormone will have strongly feminizing effects on males purely by virtue of shutting down their testicular T production (whereas girls won't have comparable feminizing effects because they have no testicles).
Quote
It will be hard to prove. Our feelings may stem for psychological reasons purely. And who cares? I don't need any of that to justify being female and transitioning. It feels right to me. End of story.
If it were known that a lot of people have ended up trans as a result of a medical mistake (and that for all trans people, it's basically a form of intersex, except one in which the main effects have been on the brain), I think it would go a long way towards reducing prejudices and increasing acceptance of transgender people. There's also the fact that medical treatment during pregnancy involving synthetic hormones and hormone disrupting drugs is still taking place, and it's highly likely that kids are continuing to be born trans as a result. Don't you think that's something that should be addressed?

